The Red Cross Magazine July 1917
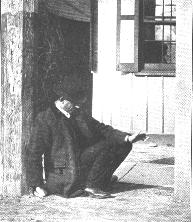
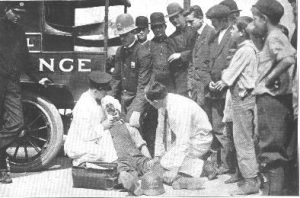
First Aid to the Unconscious
By Charles Phelps Cushing
THE surgeon, who is our chief source of information for the material contained in this series on first aid, opened his Red Cross text hook to the chapter on “Unconsciousness, and carefully checked it, sentence by sentence, for accuracy. Then he turned back to the first page, spread the hook open on his desk and reached for a pencil and a pad of note paper.
“All true to the letter,” he observed, “but I wonder if it’s all true to the spirit? Do you get the impression after reading this chapter that the diagnosis cf unconsciousness is rarely difficult if you know all the rules? Let me tell you from experience, then, that cases in this classification often baffle the most expert. Don’t get it into your head that the subject is one which is all cut and dried. Sometimes you can tell what is wrong and sometimes you can’t. Beware of feeling cocksure and never delay about calling a doctor if you have the slightest doubts about the nature of the case. In cases of unconsciousness produced by severe shocks, suffocation, poisoning, sunstroke, or bleeding, every moment is precious and you must set energetically to work yourself while the doctor is on the way. But usually the best service the first aid man can render is to make the patient as comfortable as possible and to learn as much as he can about the history and the nature of the case through close observation and inquiries.
“Note carefully a choice of words that the text hook makes in speaking of unconsciousness: ‘Perhaps no condition which the first aid student may he called upon to treat may prove more puzzling!’ Sometimes the condition is more than puzzling-it is baffling. But perhaps the point to emphasize is that to make a correct diagnosis of the cause of the knock-out is a great deal more difficult than the comparatively simple operations of administering first aid treatment. The commonest causes of insensibility number not more than a dozen -bleeding, shock, electric shock, sunstroke and heat exhaustion, freezing, fainting, fits, apoplexy (or injury to the brain), alcoholism and a few forms of poisoning.
“How to detect and how to treat cases of bleeding and of shock are matters that we have discussed before. Electric shock should carry its own evidence, and the first aid treatment is artificial respiration. The diagnosis of sunstroke, heat exhaustion and freezing should not be difficult and common sense dictates the proper procedure–do what you can to raise or to lower the patient’s temperature toward normal.
“We have on another occasion discussed fainting. It should not be necessary here to do much more than throw out a reminder that the cause is a lack of blood in the brain. Consequently, the proper treatment is not to raise the head. A hint or two from the text book is worth remembering: ‘You sometimes can prevent fainting by having the person who feels faint double over so that the head is between the knees. If this is not effective at once do not continue. Air, especially cold air, and cold water often prevent actual fainting when a person feels faint. If a patient has actually fainted, put him in a lying-down position with his head lower than the rest of his body, so that the brain will receive more blood.'”
In case of apoplexy or injury to the brain, the head and shoulders should be raised; beware of administering stimulants; place cold cloths to the head and see that the patient gets rest and quiet—preferably in a dark room.
There is little to do in a case of fits. Wrap a handkerchief around some convenient object and place patient’s mouth to prevent his injuring his tongue. Do not try to prevent the convulsions.
Of fits the surgeon had little to say except in the way of reassurance that they are not as serious as they appear to be and usually are comparatively easy to treat. They are not difficult to identify- jerking, convulsive movements of the limbs, resulting in disarranged clothing; the eyes roll; the patient may foam at the mouth and bite his tongue. “Very rarely are they fatal. There is little to do but to wrap a handkerchief around some object that happens to he convenient and place it in the patient’s mouth to protect him from injuring his tongue. Do not try to prevent the convulsions. Simply place him on the ground where he cannot bruise himself by his movements.”
The treatment for apoplexy or for injury to the brain is, from the first aid viewpoint, ticklish business. The head and shoulders must he raised, not lowered as in treating a fainting spelt. Make all speed in getting a doctor; beware of administering any stimulants; place ice or cold cloths to the head and take great pains to see that the patient gets rest and quiet-” in a dark room, if possible.” Do not make the mistake, our surgeon cautions, of supposing that apoplexy is peculiar to heavy-set persons of florid face. Even though the breath may suggest that the man has been drinking, do not make hasty surmises: “the person with apoplexy may have been drinking,” or some one in the crowd may have given him a stimulant after the accident. In handling many cases of unconsciousness you are on ground that may baffle the medical man. It is not uncommon, as our police department blotters show, for a man with apoplexy to be locked up as a “common drunk” and to die later on in a cell.
The text book gives the following description of the symptoms of alcoholic poisoning: “Perhaps evidence of intoxication. Unconsciousness partial or complete; frequently able to arouse patient to some extent. Face sometimes flushed and bloated, or may be pale. Skin cool and may be moist. Pupils natural or large. Eyeballs red, but not insensitive to touch. Breathing about as usual when in deep sleep. Pulse, usually rapid and weak, but may be slow. May he strong odor of liquor. No paralysis.”
Remember, you are dealing with a poison—the poison of alcohol—when you treat drunkenness. That is why the prescription is to cause the patient to vomit by tickling the back of his throat, or by administering an emetic of mustard and water or a large quantity of lukewarm water. The idea is to rid his body of as much of the poison as possible. But while this is the right course for alcoholism; it would cause bleeding into the brain if the patient were apoplectic.

In cases of poisoning get a doctor at once. Memorize as much as you can about the common varieties of poison and their antidotes.
In dealing with poisons other than alcohol, do not suppose that an emetic is always the best treatment. The text book put the case this way: “Nevertheless, it (an emetic) should always be given if you do not know what poison has been taken and the proper antidote.” Our surgeon’s advice is to memorize as much as you can about the common varieties of poisons and their antidotes, but to place no more dependence upon your own judgment than is absolutely necessary. The first duty is to get a doctor to the patient with the greatest haste. A little table may help to keep the classifications straight in your mind. Make one out like the one at the bottom of the page.
Making out the table will help you to memorize its facts. After you have learned them, you will not, of course, presume that this rudimentary knowledge of what to do in an extreme emergency makes you competent to dispense with the services of a doctor for poison cases. Your first duty in such cases always is to get a medical man to the patient as quicky as possible.
| Nature of Poison | Symptoms | Treatment |
|---|---|---|
| Corrosive | Burning effect on lips and mouth; stains | Best not to give an emetic where a stain is evidenced |
| Carbolic acid | Mouth burned black or white | Alcohol and water; 3 or 4 raw eggs; castor or sweet oil |
| Sulphuric acid, etc | Mouth burned black or white | An alkali, such as baking soda |
| Strong alkalies | Mouth burned black or white | Give vinegar, lemon or orange juice |
| Irritent poisons (Such as Paris Green) |
Do not stain lips, etc. | An emetic and stimulants required. |
| Nerve poisons Opium, morphine, laudanum, etc. |
Do not stain. Pupils of eyes very small; sleepiness, later insensibility, etc. | Require an emetic; keep patient awake and moving if he is strong enough. Slap with a wet towel; administer hot strong coffee. |